I am a medical dosimetrist, and when I opened the dose map for a breast cancer patient, I realized my fiance had been shortening radiation treatments by changing the plans after the doctors approved them.
I am a medical dosimetrist, and when I opened the dose map for a breast cancer patient, I realized my fiance had been shortening radiation treatments by changing the plans after the doctors approved them.
My name is Brenda Malone. I build radiation plans, and Gary Fenton forgot the machine keeps its own memory.
Let me tell you what this work is before I tell you what Gary did.
Dosimetry is the architecture of harm reduction. Radiation oncology delivers lethal doses to tumors and tries not to kill the things around them. My job is to engineer that boundary—build a plan from the CT scan and the oncologist’s prescription, shape the beam angles and weights and margins until the dose-volume histogram shows the tumor getting what it needs and the spinal cord and salivary glands getting as little as possible. Physics defines the constraints. I find the plan that satisfies them.
It is not intuition. It is not art. It is geometry and calculation inside a tolerance window, and when the physician signs the plan, the signature means: this geometry is the treatment. Nothing changes after that signature without a new approval.
Last week I spent three hours refining a head-and-neck plan for a sixty-two-year-old named Mr. Elliot. The oncologist wanted ninety percent of the prescribed dose to cover the tumor volume while the parotid gland—the salivary gland behind the jaw—stayed below twenty-six gray. The first iteration missed that threshold: parotid mean dose was 28.1 gray, high enough for permanent dry mouth. I pulled the plan back into the optimizer and adjusted the beam weights, shifted an arc, brought the parotid mean to 24.8 gray without compromising tumor coverage. Three hours for 1.4 gray of margin. The resident watching over my shoulder asked if the difference was clinical.
I told her: yes. At 26 gray, forty percent of patients have measurable salivary function loss at two years. At 24, the number drops. The clinic’s job is to give every gray that matters and not give the ones that don’t.
She wrote that down. Then she asked: “Do patients understand that margin when you explain the plan to them?”
I told her: “Sometimes. I explain what the plan is protecting. The oncologist explains the full picture. My job is to build the geometry that makes the oncologist’s picture possible.”
She asked if I found it frustrating when patients didn’t understand what I did. I said no—patients aren’t required to understand dosimetry. They’re required to receive the dose the physician prescribed. My job is to make that happen, and the metric of success is in the delivery log, not in the patient’s ability to describe parotid sparing.
She wrote that down too. Residents write down things that seem cold until they realize they’re just precise.
The same morning I caught a couch-angle discrepancy before treatment began. The therapist had entered the couch rotation in the wrong field—the plan specified negative seven degrees, the console showed positive seven. The difference between negative seven and positive seven on a couch angle is fourteen degrees of beam entry error; for a pelvic plan, fourteen degrees can place the dose centroid well outside the target volume and into the femoral head.
I said: “Hold.” I said it the way I always say it—flat, not alarmed, the word a technical signal not an indictment—and the therapist stopped, checked the field, saw the sign error, corrected it. I did not make a report. I made a note. The system logs all treatment start delays. That log is evidence.
That is how radiation safety works: every action leaves a record.
The therapist thanked me afterward—quietly, in the hallway, not in front of the patient. She said: “I don’t know how you saw it that fast.” I told her: I look at the console before every beam start. Not because therapists make errors—they rarely do—but because the cost of one uncaught sign error is higher than the cost of one extra thirty-second check, every time. Fourteen degrees. Every fraction. Over six weeks.
She nodded in the way people nod when they understand the math and don’t enjoy it. I understand the not-enjoying it. The math is what it is.
Gary brought coffee into the planning room on a Tuesday and said I “see math where other people see hope.” He said it fondly, the way he said things about my work that were slightly condescending and dressed as compliments. He had been running the clinic’s operations for four years. I had been at the clinic for two. We had been engaged for seven months.
He set the coffee beside my monitor and read the dose-volume histogram on screen. He said: “The trick is keeping the lights on long enough to use the physics.”
I said: “The physics doesn’t need lights.”
He smiled and left. The coffee was the right temperature. The plan on my screen had a parotid at 24.8 gray. I did not audit Gary’s email calendar that morning.
The arsenal seed had been planted eighteen months earlier when I passed the American Board of Radiology dosimetry exam and accepted this position. The machine at this clinic—a Varian TrueBeam—records a complete delivery log every fraction: gantry angle, collimator setting, monitor units delivered, beam-on time. The delivery log is stored separately from the treatment planning system. The delivery log does not care what the plan says. It records what the machine did.
A signed approval is not the end of a radiation plan. The machine records what it actually delivered.
The surface crack was a complaint from a patient named Mrs. Theodosia Wells.
She had finished a six-week breast protocol and was waiting for a follow-up. She mentioned to the receptionist—offhandedly, in the way patients mention things they expect to go nowhere—that one of her early sessions had ended six minutes early. The machine had stopped. She’d been told it was a calibration check. She hadn’t worried about it then. She was mentioning it now because she was nervous and nervous people look back.
The receptionist left a note. The note reached the front office coordinator. The coordinator filed it in the patient comment folder—a manila folder in a filing cabinet that nobody treated as urgent.
Gary pulled the comment folder on Thursdays as part of his operations review.
I found out about the complaint the same way I found out about Gary’s expansion budget requests: he mentioned it at dinner, framing it as a workflow problem he had already resolved.
I said: “Which patient?”
He said: “Mrs. Wells. She’ll be fine. The machine did a check cycle.”
I said: “What plan?”
He said: “Breast. Your plan.”
That was Thursday. Friday morning I pulled Mrs. Wells’s file.
I had built her plan in October. The oncologist had prescribed forty-five gray in fifteen fractions—three gray per fraction, five days per week, three weeks. I had designed an opposed tangential field arrangement with a slight field-in-field technique to reduce hot spots. The physician had approved the plan. I had signed the physics check. The plan was clean.
I exported the DICOM RT Plan file from the treatment planning system. DICOM is the standard format for medical imaging; RT Plan files contain every beam parameter, every monitor unit, every fractionation schedule that defines the plan as approved.
The plan I found in the archive matched the October approval exactly.
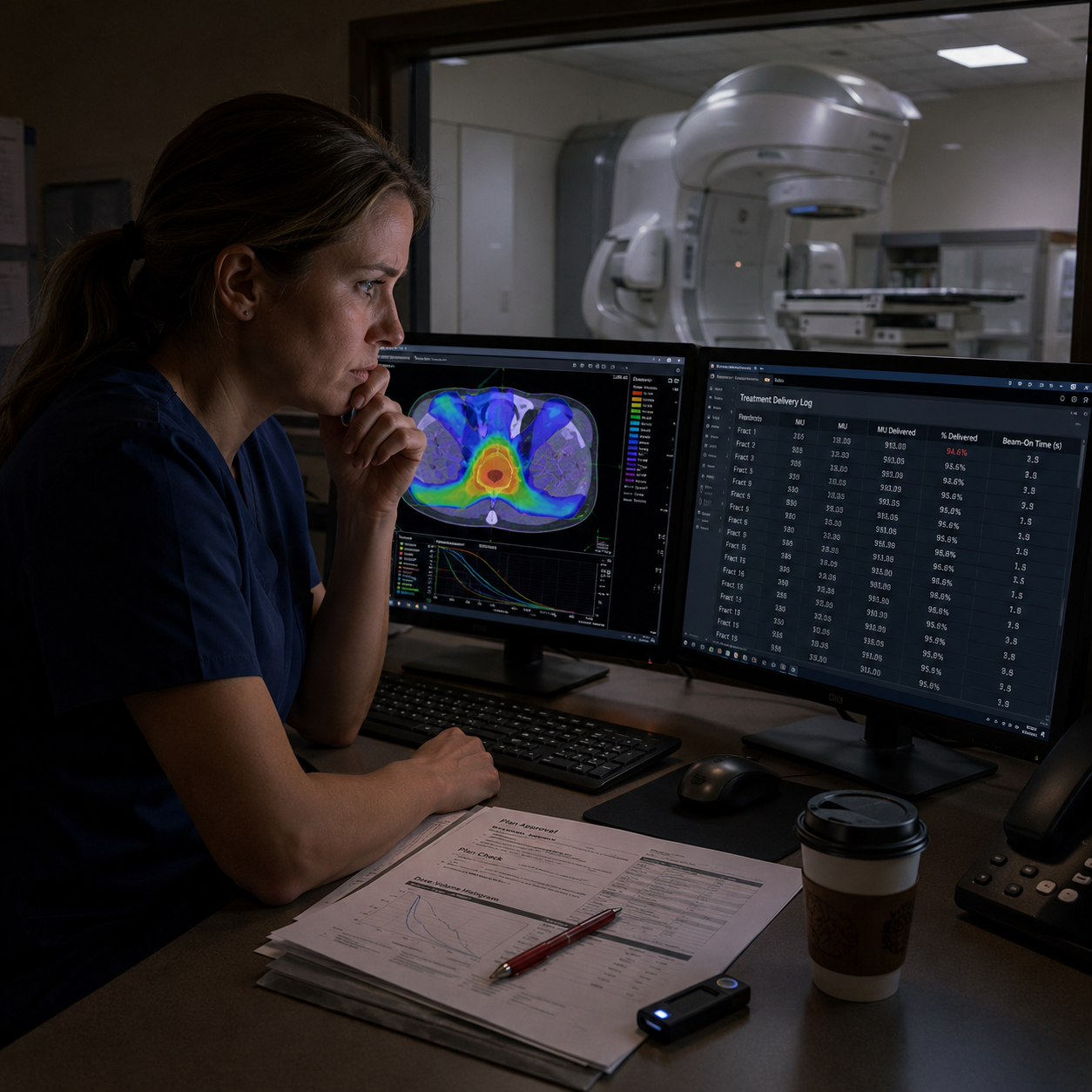
Then I pulled the delivery logs from the TrueBeam console.
Fraction three.
The monitor units delivered in fraction three were 94.6 percent of the fraction prescription. Not 100 percent. Not a check cycle. A shortened delivery—beam cut before the full monitor unit count completed.
I sat with that number the way I sit with dose-volume failures: not panicking, just calculating. 94.6 percent of three gray is 2.838 gray. One fraction, 0.162 gray short. Over fifteen fractions, if every fraction ran at that rate, total dose would be approximately 42.6 gray instead of 45. Cumulative under-dose approaching six percent.
I printed the delivery log. I opened the DICOM archive again and sorted by modification date.
The DICOM file had two version timestamps. The creation timestamp matched October—the date I built the plan. The modification timestamp was six days after physician approval.
Someone had opened the plan after approval and saved a change.
I pulled the audit log from the treatment planning system. The system logs every access by user credential. The modification on day six was logged under a credential I did not recognize—a technical administrator account.
Gary administered the technical administrator accounts.
I printed the dose-volume histogram. I capped my red pen. I called Dr. Priya Mehta, the independent medical physicist who had trained me three years ago and who now consulted for clinics without full physics staffing. She had never worked at this clinic. She owed Gary Fenton nothing.
I told her what I had: delivery log showing 94.6 percent monitor unit delivery in one fraction, a DICOM file with a post-approval modification timestamp, an audit log entry under a technical administrator credential. I described the numbers without naming anyone. She said she could look at exported files by the end of the week. She asked if I had pulled delivery logs for other patients in the same window.
I said I was doing that now.
She said: “How many are you expecting?”
I said: “I don’t know yet.”
She was quiet for a moment—the particular quiet of an experienced physicist who is running the implications. She said: “Get me the files before Sunday. Call me if you find more than one.”
I said: “I need to know before Sunday. There is a server migration scheduled for 21:00 Sunday night.”
I had seen the migration in Gary’s email calendar because Gary and I shared a household calendar and he had copied clinic logistics to it for scheduling reasons. The migration was an IT infrastructure upgrade—new server architecture, old planning system data migrated to new storage. Standard procedure. Normally irrelevant.
Except: server migrations sometimes change file metadata. A modification timestamp in a migrated file is not guaranteed to transfer intact. If the original planning server was decommissioned after the migration, the evidence of when the plan was changed would become unverifiable. The audit log would still exist—the treatment planning system logs were separate from the file system—but the DICOM file timestamp that corroborated the log would be gone.
21:00 Sunday was the hour the original version could be overwritten.
I did not tell Gary what I had found. I told him I was working on a QA backlog and would be at the clinic late Friday.
In March, four months before the Mrs. Wells complaint, the clinic had treated thirty-eight patients in a week that typically ran twenty-two. Gary had requested the additional throughput as part of a grant application—rural oncology volume data for a federal rural health grant. He had presented the proposal to the board with a slide that showed patient access statistics and a regional map of the nearest competing oncology center: ninety miles. He used the ninety miles the way politicians use statistics—not as data, as a closing argument.
I had flagged the March schedule as aggressive for the physics staffing level. Two dosimetrists, one physicist, one clinical director, thirty-eight active treatment courses: the math said someone would be at capacity. Gary had said: “Rural clinics have to be flexible or they close.” He’d said it with the patience of a man explaining something obvious to someone technical.
I had accepted the frame of that argument because the alternative—that the flexibility was not about access but about numbers for a grant—required me to believe something I wasn’t ready to believe in March.
I had not audited the delivery logs for those thirty-eight patients.
In January, before Gary’s operational expansion proposals had gathered momentum on the board, a radiation therapist named Sandra had mentioned in passing that Gary had “adjusted some session lengths to fit the schedule.” I had asked what she meant. She said he had told the console operators that certain plans had built-in check cycle buffers that could be shortened without dosimetric impact. She had used the word buffers. Gary had used the word buffers. Buffers is a word that sounds technical enough to discourage follow-up questions from people who don’t work in treatment planning.
I was the person who worked in treatment planning. I did not ask a follow-up question.
Sandra had assumed it was a technical matter she didn’t understand—that Gary had explained something to the console operators that fell outside her training. She had not filed a report. She had mentioned it to me because she trusted me and because it had bothered her in the low-key way things bother technicians who don’t have authority to name what they see but have enough experience to know when something doesn’t fit.
I had asked Gary about it that evening. He said Sandra sometimes misunderstood operational communication. He said the machine’s tolerance windows accommodated minor session length variation. He used the phrase “tolerance windows” the way he had used “buffers”—technical vocabulary as argument, deployed to end a conversation with someone technical enough to understand the words but trusting enough to accept them without verification.
He said nothing that was technically false and nothing that was completely true, and I had accepted the frame of his answer because I had trusted the architecture of our household the way I trusted a plan that was signed.
The plan was signed. Someone had edited it after. Sandra had mentioned the buffers. I had asked Gary. He had reframed. I had accepted.
That sequence is what I carried forward from January into May when Mrs. Wells’s complaint arrived on Gary’s Thursday operations folder. I did not carry it as proof of anything—I carried it as a thing I had filed under “resolved, Gary’s explanation” without verifying the resolution against delivery logs.
The delivery logs don’t care what explanation Gary gave me in January.
On Friday evening I returned to the clinic at 7:15 PM. The treatment rooms were empty. The TrueBeam vault was locked for the night—the heavy doors sealed, the warning light above the entry dark. The planning room still had three monitors running in screen-saver mode, the dose-volume display cycling through a background render.
I logged in under my own credentials. I did not use the technical administrator account. I used mine—my name, my certification number, my login timestamp—because everything I was about to access needed to be traceable to an authorized user with a documented legitimate purpose.
I pulled delivery logs for every patient treated in the six-week window around Mrs. Wells’s protocol. Then I expanded the window to the full five-month period Gary had mentioned the March scheduling increase. Then I went back to the beginning of the grant-period data: fourteen months.
Eleven patients showed delivery log discrepancies. Not all eleven showed the same magnitude—fractions ranging from 2 to 8 percent under-delivery, some scattered across treatment courses, some clustered in specific weeks. The clustering pattern corresponded to weeks when the treatment schedule was above the clinic’s standard capacity. High-volume weeks. Grant-documentation weeks.
All eleven had plan modification timestamps in the same window: three to twelve days after physician approval, under the technical administrator credential. Same account. Same post-approval pattern. Same window between physician signature and modification.
I sat with that pattern for four minutes before I began the export. Four minutes because I had been engaged to Gary Fenton for seven months, had lived with him for two years before that, had trusted his understanding of this clinic’s operational pressures, had accepted the frame of “flexibility” as a reasonable response to rural resource constraints.
The frame was the plan. The plan was altered after it was signed. The machine did not care about the frame.
I exported all eleven DICOM RT Plan files to an encrypted USB drive I had brought from home. I exported the delivery logs. I exported the treatment planning audit log covering the fourteen-month window. I photographed the console screen with the log timestamps visible—the physical screen capture that would corroborate the digital exports if anyone later questioned whether the timestamps had been manipulated before I accessed them.
At 8:41 PM I emailed Dr. Priya Mehta with the encrypted file attachment and a decryption passphrase in a separate message.
At 8:55 PM I called the State Radiation Control Program’s after-hours line and left a message with the incident summary and my contact number.
At 9:03 PM I began drafting the report to the clinic’s accrediting body.
Gary called at 9:12 PM. He asked if I was still at the clinic. I said yes. He said: “The migration is tomorrow night. The IT team needs access confirmation before noon.” His voice was ordinary. Planning voice. The voice of a man who did not yet know the audit log had been read—who was still operating under the assumption that the migration would run on Sunday, the old server would be decommissioned, and the file timestamps would not transfer intact to the new system.
I said: “I’ll send a note to IT.”
I did not send a note to IT. The state radiation program’s incident report was already logged. The accrediting body notification was in my sent folder. The evidence was on an encrypted drive in my bag. The server migration would be stopped by the state hold before Gary’s IT team ran the first file transfer.
I finished the accreditor draft at 10:20 PM. I drove home. I passed three traffic lights and a pharmacy that was still open with its sign lit in blue and I thought about the difference between the Gary who brought coffee into the planning room and said I saw math where others saw hope, and the Gary who had understood machine time as a budget line while the coffee was still warm.
Those were not different Garys. That was one Gary.
I did not delete Gary’s coffee cup from the planning room counter.
The board meeting was Tuesday morning at nine.
Gary had prepared a twenty-four-page expansion packet: patient volume projections, rural health grant eligibility, a line-item equipment budget for a second linear accelerator. The board chair, Martin Okafor, had read the executive summary before arriving. Three of the five board members had clinic administrative roles. One was the medical director. One was the community health representative, a retired school principal named Constance Beard.
Dr. Priya Mehta had driven two hours for the meeting. She sat beside me with a manila folder containing her preliminary variance analysis.
The State Radiation Control Program had called back at 7:30 that morning and confirmed receipt of the incident report. They had issued a preliminary notice requiring the clinic to preserve all treatment planning data pending investigation—the migration had been halted by order of the state program before 21:00 Sunday. The original planning server was under evidence hold.
The 21:00 migration—the hour Gary had chosen to upgrade the infrastructure—became the hour the evidence was sealed instead.
Gary stood at the projection screen with his expansion packet displayed. He said: “This year represents a turning point for rural oncology access in this region.” He was wearing the navy jacket he wore to external presentations—the one he called his “board jacket,” which he kept in a separate dry-cleaning bag from the rest of his suits. He had dressed for the presentation he had prepared. He did not look at me when he entered the room.
Martin Okafor said: “Before we proceed to new business—Brenda, you requested time at the opening.”
I said: “Yes.”
I stood. I placed the summary sheet on the table—one page, clinic letterhead, the eleven patient records, the delivery log variances, the plan modification timestamps, the accreditor notification number, the state program incident case number issued that morning. One page. I had drafted it three times to make it one page.
I said: “Over a five-month period, eleven patient treatment plans were modified after physician approval under a technical administrator credential. The modifications reduced monitor unit delivery in individual fractions. I have reported this to the state radiation control program and the accrediting body. The state program has placed a hold on the planning server pending investigation.”
Gary said: “You are misunderstanding operational adjustments.”
I said: “The doctor approved 50 gray. The machine delivered 44.”
The board members looked at the summary sheet and then at Gary and then at the summary sheet. They were not physicists, but they understood that a physician-prescribed number and a machine-delivered number were different numbers, and that the difference had a patient attached to it.
Gary said: “No one was harmed.”
I said: “You do not know that.”
A silence settled in the room—the kind that happens when someone has said the definitively true thing and the room is waiting for the weight of it to distribute.
Dr. Mehta slid the variance report across the table—two pages of independent analysis, her board certification number in the header, each patient’s deviation expressed in gray and in percentage. She said: “Independent verification of eleven treatment plans is consistent with the delivery log evidence. The magnitude of under-dose in three cases warrants immediate oncology review.”
The chief radiation therapist, Sandra, covered her mouth with both hands.
Martin Okafor closed Gary’s expansion packet. He did it slowly, with both hands, the way you close something you want to be seen closing.
Constance Beard said: “What does ‘patient recall’ mean for these families?”
Dr. Mehta said: “It means their treating oncologists review whether the treatment course was clinically sufficient. In most cases the answer may be yes. In some cases the physician cannot promise that.”
Constance Beard wrote something on her notepad. She underlined it.
Gary said: “I kept this clinic open. The grant required volume.”
Martin Okafor said: “Gary. Stop.”
He said it the way chairs say stop when they have made a decision and the decision is not a discussion. He turned to the compliance officer, a man named Warren Keith, and said: “Secure the planning server. Escort Mr. Fenton from the building.”
Gary looked at me once. Not wounded, not angry—a flat, calculating look that measured how far the evidence had traveled from the delivery log to this table. He had believed the migration would remove the timestamp corroboration before anyone asked to compare it against the audit log. He had believed I was technical in a way that was useful to him rather than dangerous.
He understood it had traveled all the way.
Warren Keith opened the boardroom door.
The chief therapist’s hands came down from her mouth. She exhaled in the particular way people exhale when they have been waiting to stop pretending something is normal—when the performance of normalcy is released and the real shape of the situation is allowed to stand.
The patients were recalled beginning Wednesday.
Patient eleven—a man named Harold whose lung protocol had run eight percent short across twelve fractions—was seen by his oncologist that afternoon. His most recent imaging was stable; the oncologist could not promise that the under-dose had not mattered, but the imaging did not show early treatment failure. She said she would watch carefully. Harold asked what watching carefully meant. She said: more frequent scans, closer follow-up intervals, less margin for error at the next review.
Harold asked what watching carefully meant. She said: more frequent scans, closer follow-up intervals, less margin for error at the next review. She said it plainly. She said it the way oncologists say things when they cannot offer certainty and will not pretend otherwise.
Harold nodded the way patients nod when they are processing a risk they had not been told they were carrying—when they are calculating how many ordinary Tuesdays and ordinary phone calls had passed between the day the treatment ran short and this afternoon, and whether any of those Tuesdays had been the one where the difference mattered.
I was not in the room when Harold received that conversation. Dr. Mehta told me about it afterward in the parking lot, standing beside her car with a folder under her arm, the afternoon light on the concrete making everything too flat and ordinary-looking for what we were talking about.
Mrs. Theodosia Wells’s oncologist reviewed her film and reported stable margins. She said the six-percent cumulative deviation was within the range where clinical outcomes often diverge at five-year follow-up, not immediately. She said the word often carefully. She did not say always. She noted the case for accelerated follow-up at twelve and eighteen months.
Mrs. Wells had mentioned the six-minute session offhandedly to a receptionist because she was nervous. That offhand mention was a patient complaint filed in a manila folder in an operations cabinet. The complaint had worked its way to Gary’s Thursday review folder, and then to his dinner table as a workflow note he had already resolved.
He had not resolved it. He had given it a frame.
She had not known she was filing evidence. She was just nervous, and nervous patients look back.
The eleven recalled patients were seen over the following four business days. Their oncologists reviewed imaging, treatment records, and the variance analysis Dr. Mehta had prepared. In seven cases the treating physician was able to say the clinical outcome was likely unaffected—tumor response imaging was consistent with adequate dosing and the under-delivery fell within the range where disease control probability remained high. In one case the answer was more cautious. In three cases the physician used the phrase “we will watch carefully,” with all the weight that phrase carries when it is the most honest thing available.
Each of those conversations happened in an exam room I was not in. I wrote the reports. The oncologists delivered the news.
I had built all eleven of those plans. I had checked the physics, verified the dose-volume histograms, watched the physician signatures appear in the planning system. I had not watched the modification timestamps that appeared afterward. The gap between what I verified and what the machine delivered was the gap Gary had operated in for five months.
I did not feel absolved by the fact that I had found it. Finding it was the job. The job started earlier than it had.
I was in the treatment vault the evening after the board meeting. The room was quiet in the particular way shielded rooms are quiet—not silent, because the ventilation system maintains positive pressure, but insulated from the clinic sounds outside. The TrueBeam sat in its rest position, gantry at zero, the beam stopper engaged.
At 21:00 the machine powered down under state order. The technician on duty locked the console and handed the key to the compliance officer, who logged it as evidence.
21:00. The hour Gary had scheduled for deletion.
The hour the evidence was preserved instead.
I placed a fresh QA sticker on the control console housing—a small adhesive calibration tag, the kind we apply after every monthly output check. I did not sign it. The next physicist who completed the formal QA would sign it. I was not that physicist right now. I was the person who had found the gap between what the plan said and what the machine delivered, and I had done what the job required.
The treatment vault was clean and quiet and would accept another patient when the state review completed and the plans were re-verified and the new approvals were signed. The machine did not know what Gary had done to the plans. The machine knew only what it had delivered, and it had logged every fraction, and the log was intact.
Gary treated minutes as money. He had understood machine time as a budget line and under-delivery as a rounding error invisible to review. He had understood the treatment planning system as a soft target—editable, administrator-accessible, not watched by the person whose credentials were on the approved plan. He had understood my competence as a resource to use and my audit habit as something that would not reach backward through five months of delivery logs without a patient complaint to trigger it.
He had been approximately correct for five months.
I knew minutes could be medicine. Six minutes per fraction, eleven patients, five months—not rounding error. An accumulation with eleven names and eleven oncology charts and eleven follow-up schedules that were now longer and more frequent than they should have been.
The machine had recorded every fraction. The machine had not flagged the discrepancy because the machine delivers what the plan file tells it to deliver, and the plan file had been changed before the machine saw it. The machine was doing its job. The machine needs a human to compare what the plan authorized against what the file says.
That comparison is my job. The machine keeps its memory. My job is to read it.
The vault door was heavy and slow when I pushed it open to leave. The hallway outside was ordinary clinic light—fluorescent, functional, the same light the patients walk through when they come for treatment. I pulled the door until it sealed.
The QA sticker on the console was unsigned.
It would stay unsigned until someone completed the work honestly. Not until the investigation resolved, not until a license was reviewed, not until a lawsuit was filed or settled or appealed. Until someone ran the machine through a full calibration protocol with documented output measurements and a physicist’s signature that meant: this machine has been verified, these outputs are accurate, the plans this machine executes can be trusted.
That work would happen. The state review would clear the machine when the machine was cleared to clear. The new plans would be approved by physicians who had been told what the old plans were missing. The next patients would receive the doses their oncologists prescribed, measured by a machine that had been logging every fraction honestly for fourteen months while the plans above it were changed.
The machine did its job. It always did its job.
That is the only kind of completion the machine accepts.